Let's begin explaining the original situation, a catastrophic result arisen after a botched surgery done elsewhere to a patient born with severely tuberous or tubular breasts, very slim, actually skinny due to her passion for practicing intensively sports, to whom no tuberous breast correction was applied thus leaving intact the conical shape and the enlarged and herniated areolas; furthermore the submammary crease, typically too high in tuberous breasts, was not lowered as it is mandatory in all such cases, leading to eccentric implants riding too high in patients chest, nipples gazing down and a waterfall effect of the breast mounds; additionally the implants had been placed totally under the muscle of the pectoralis, something against all principles of good practices in breast implants surgery, which lead, actually always does, to a muscle flex deformity also called animation deformity or elevator breasts, forming a grotesque deformity visible in the images by contracting the pectoralis muscle.
The patient's frame was very slim and skinny, being such features an augmented risk factor in every breast surgery, much more in revision mammoplasties like this one; she did not seek or request a major increase in volume, opting for similar breast size but using anatomical shaped implants unlike the round or spherical she was carrier of.
The surgical plan included areolar reduction to downsize its perimeter and flatten it in, tuberous breast correction with plasties, total capsulectomy and removal of the obsolete implants from underneath the muscle and building a subfascial plane pocket to insert the new anatomical contour implants, associated with a well calculated lowering of the submammary crease; a multipoint capsulorrhaphy had to be applied to close and reduce the prosthetic pocket which exceeded the outer end of the left breast, also called side boob deformity, and on the inner quadrants of the right breast, since there was certain symmastia; complementarily the inner quadrants of the left breast and the outer side of the right one had to be expanded, plus the submammary crease lowered, all that to achieve centricity of the implants according to the nipple areola complex.
This procedure turned out very successful initially, in spite of its difficulty and the awful condition of the tissues; however shortly after the breasts initiated a partially unfavorable course of evolution which, once stabilized, still provided an awesome improvement and nicely shaped breasts, but not the most optimal result possible due to two issues arisen; firstly the right breast evolved to a slight bottoming out effect migrating inferiorly and medially to a certain eccentricity from the ideal according to the nipple areola complex, due to the flaccidity and the poor healing properties over the implant which failed to form strong adhesion to the ribcage, aggravated by the weak and thin skin support under the prosthesis; to the contrary, the left breast experienced a kind of partial capsular contracture and pinching of the lower and outer quadrants, forcing its migration superiorly and medially, leaving the inferolateral quadrant totally empty.
The situation was way better then the disastrous initial situation, actually was an optimal result but neither an perfect one; in these borderline scenarios it will always depend on patient's perfectionism and goals if a new revisional intervention should be done or not, given the breasts looked nice and significantly improved; of course, a new intervention is feasible and judicious only if the surgeon is able to deal with it at very high technical performance.
This patient had high expectations, realistic but perfectionist, and the surgeon felt totally capable and comfortable to meet her goals, so a new revision mammoplasty was planned; additionally she began to change her mind, expressing her wish to go this time for a very large breast volume and, instead of anatomical and aware of the fake look she'd get with them, getting round or spherical shaped profile implants, perfectly warned of the ball effect they entail.
A new revision procedure was scheduled to redefine the subfascial pocket to the width and base of the new implants of significantly larger volume, applying a new set of pocket closures by means of capsulorrhaphy and also expansions so that the centricity of the nipple areola complex is achieved at the very right peak of the prosthetic mound or maximum projection point; the areolas were also revised.
Finally and after two extremely difficult surgeries the patient has achieved the goals she sought, is happy with the size and shape of the breasts and all the initial issues have been totally eradicated; however many patients might have well preferred anatomical shaped implants, especially if they are slim or seeking large volumes, to achieve a more natural looking result and better upper pole fullness exempt of hollow areas and steps.
This case is a lesson to those surgeons and patients who are prone to trivialize revision surgeries of the breast; revision mammoplasties may be unrewarding the first attempt, but if the patient is really motivated, the surgeon skilled enough and both stubborn and perfectionists, a very successful and happy outcome is possible.
Note: the patient underwent two revisional procedures, therefore the images are sorted first in order as before and after of the first breast revision, comparing the initial catastrophic result, including some images contracting the pectoralis to show the animation deformity, with the outcome of the first attempt of repair; the second in timely order are the before and after images comparing the situation previous to the second revisional procedure and the very final result; the third series of images compares the catastrophic initial before and the latest and best outcome obtained after both revision mammoplasties.
READ LESS

























 Sending vote...
Sending vote...

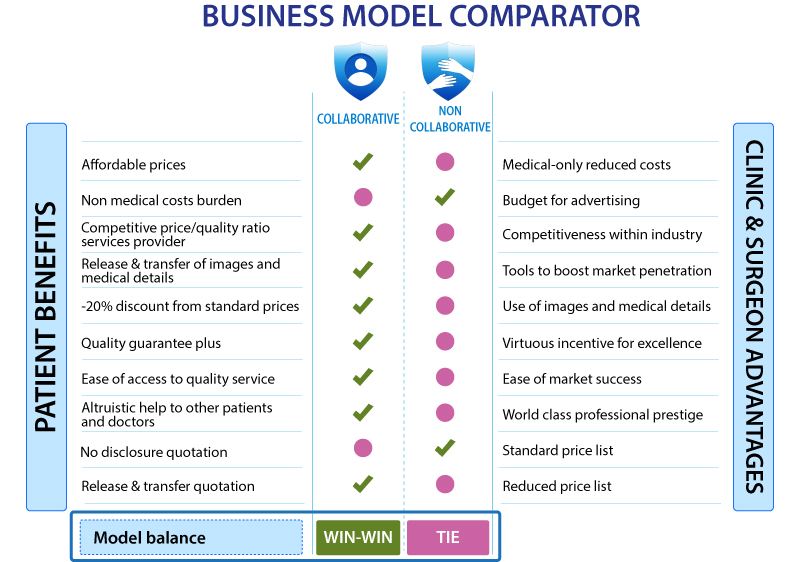
 READ MORE ABOUT BENEFITS OF THE COLLABORATIVE MODEL
READ MORE ABOUT BENEFITS OF THE COLLABORATIVE MODEL

 +34-900-838448
+34-900-838448 +44-0-800-0488400
+44-0-800-0488400 +1-844-4000840
+1-844-4000840






















































































































































































































































































































































































































































